MOTS-c
MOTS-c is a small peptide made inside your own mitochondria. Your body produces less of it as you age, and exercise is the most reliable way to increase it naturally. Researchers have studied it for metabolic health, insulin sensitivity, and age-related decline. We read the evidence plainly, set expectations honestly, and only consider it for patients whose full clinical picture makes sense.
Compliance Notice: Important status notice. MOTS-c is not FDA approved for any therapeutic use. It is on the FDA Category 2 restricted list, which means licensed compounding pharmacies cannot prepare it. Any use at Paragon is research-informed, under direct physician supervision, and only after a full clinical review. The only completed human trial used a modified version of MOTS-c developed by a company that has since discontinued operations. No Phase 1 safety trial has been completed for native MOTS-c.
WADA prohibition. MOTS-c was added to the WADA Prohibited List on January 1, 2024 under the S0 category (Non-Approved Substances) and appears on the 2025 list as an example under S4 (Hormone and Metabolic Modulators). It is prohibited at all times, in and out of competition, in every WADA-regulated sport. If you compete at any level in a WADA-regulated sport, MOTS-c is not appropriate for you. Do not use it.


Overview
MOTS-c is a peptide your mitochondria produce and release into circulation. It acts as a signaling molecule, telling the rest of your body (especially skeletal muscle) to take up glucose more efficiently and use energy better. It is one of the ways your mitochondria communicate with the rest of you, and it is part of why exercise improves metabolic health.
Two things about MOTS-c are unusually well characterized for a peptide this young in the literature. First, your blood levels of it decline with age, and patients with obesity and metabolic disease have lower levels than healthy controls. Second, exercise acutely raises both muscle and circulating MOTS-c, with skeletal muscle levels increasing nearly twelvefold during and after exertion. That is a clear biological story. As you get older and more sedentary, your own MOTS-c drops, and that drop tracks with metabolic decline.
The therapeutic idea is to supplement the peptide in patients whose endogenous signaling has fallen off. The idea is compelling. The human outcome data to support it is limited, and we say so up front.

CHEMICAL STRUCTURE & PROPERTIES
- Origin: Mitochondrial-derived peptide; encoded in the mitochondrial 12S rRNA
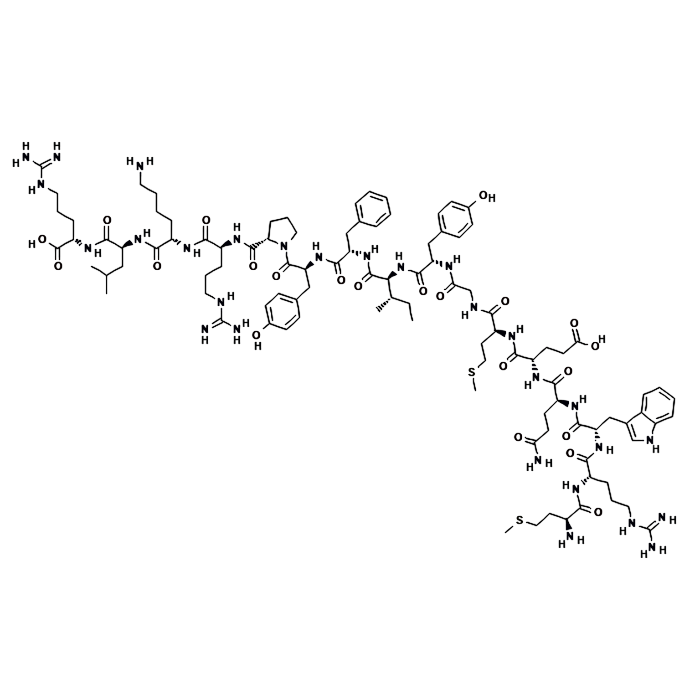
- Amino Acid Length: 16 residues
- Sequence: Met-Arg-Trp-Gln-Glu-Met-Gly-Tyr-Ile-Phe-Tyr-Pro-Arg-Lys-Leu-Arg
- Primary Target: AMPK (AMP-activated protein kinase)
- Natural Trigger: Exercise; declines with age and metabolic disease
- Route: Subcutaneous injection
- Stability: Lyophilised powder; store at 2 degrees C to 8 degrees C before reconstitution
- WADA Status: Prohibited -- S0 and S4 (2024 onward); not for competitive athletes
Mechanism of Action
Clinical Applications and
Research Evidence

Current Clinical Evidence
Safety Considerations
Regulatory Status and
Legal Considerations
Global Regulatory Status
- MOTS-c is not FDA approved for any therapeutic indication
- MOTs-C was previously on the FDA Category 2 restricted list. As of April 22, 2026, it is listed as Nominated but Withdrawn from Category 2
- The Category 2 prohibition has been lifted as of April 22, 2026. Standard 503A/503B pharmacy regulations now apply. Consult current FDA guidance and legal counsel before compounding.
WADA Anti-Doping Status
- MOTS-c was added to the WADA Prohibited List on January 1, 2024 under S0 (Non-Approved Substances)
- It also appears on the 2025 list as an example under S4 (Hormone and Metabolic Modulators, AMPK activator category)
- Prohibited at all times, in and out of competition, in every WADA-regulated sport
- If you compete at any level in a WADA-regulated sport, we will not prescribe it and you should not use it from any source
Legal Availability
- Research use of MOTS-c is legal in the United States for non-competing adults
- It is not approved as a therapeutic, which is a different question from legality
- Any use at Paragon is research-informed and under direct physician supervision
- Source, quality, and chain of custody are discussed during your consultation
Administration and Dosing
Considerations
How It Is Administered:
- MOTS-c is administered by subcutaneous injection in cycles
- Specific dose, frequency, and cycle length are determined by your clinician based on your labs, goals, and the most relevant published research
- We do not publish a standard dose on this page -- research protocols vary, and a number appropriate for one patient is not appropriate for another
- With a compound that is WADA-prohibited and that has no completed Phase 1 trial for the native peptide, self-prescribing is particularly inadvisable
Clinical Considerations:
- Your written protocol is built during consultation and includes clear instructions, a monitoring schedule, and a plan for what we measure and when
- Most patients asking about MOTS-c have more upstream work available to them -- we will tell you that if it is true
- We do not prescribe a peptide as a shortcut around foundational metabolic work
- Professional oversight is required throughout the protocol period
.webp)
How Soon Will I Feel a Difference:
- Metabolic changes on labs (fasting insulin, HbA1c, glucose handling) have their own timeline depending on your baseline
- Body composition changes, if they occur, reflect the underlying metabolic shift rather than a direct fat-loss mechanism
- We do not promise exercise-equivalent outcomes in humans because that is not what the human evidence shows
- We will set specific expectations based on your labs and goals before anything begins
Measurable Outcomes:
- We track fasting insulin, HbA1c, glucose handling, body composition, relevant lipid markers, and your own subjective report
- Metabolic health is mostly built, not prescribed -- resistance training, Zone 2 cardiovascular work, protein-prioritized nutrition, sleep, and stress management are the foundation
- A peptide is a lever, not a substitute; your plan reflects that because that is what works
- Longer telomeres on a commercial test is not the same thing as a longer healthspan, and the same honest framing applies here

Conclusion
See whether MOTS‑c fits your plan.
At Paragon, every plan begins with a process designed to cut through the noise and focus on what truly matters for your health. We start with a full intake, a careful review of your current labs, and an honest conversation about your goals—both the outcomes you hope to achieve and the evidence that will guide us there. From that foundation, we evaluate the tools available. MOTS‑c is one option, but it is never assumed. If it proves to be the right fit for your physiology and aligns with the changes most likely to move the needle for you, we will recommend it with clarity. More often, however, there is foundational work to be done first—steps that create the conditions for real progress—and we will tell you exactly what that looks like.
Our role is not to chase the latest compound, but to help you build a plan that is grounded in evidence, tailored to your biology, and focused on sustainable change. Every recommendation is made with transparency, precision, and a commitment to guiding you toward the interventions that matter most for your long‑term health and resilience.
MOTS-c SCIENTIFIC
DATA SUMMARY
Peptides work best as one part of a complete, medically supervised plan. These are often used alongside our medically supervised weight loss program in Atlanta. To see how this fits your goals, explore our full approach to peptide therapy in Atlanta.
Disclaimer: This information is provided for educational purposes only and does not constitute medical advice. MOTS-c is not FDA approved for any therapeutic indication and is classified as Category 2, meaning it cannot be prepared by licensed US compounding pharmacies. MOTS-c is prohibited under WADA S0 and S4 categories and must not be used by anyone competing in a WADA-regulated sport at any level. Any use at Paragon is research-informed and under direct physician supervision, for non-competitive adults only. Patients should consult with a qualified clinician and ensure regulatory compliance before considering any use of MOTS-c.
Explore Peptide Therapy at Paragon
Peptides work best as part of a bigger plan, not on their own. At Paragon Sports Medicine in Atlanta, every peptide is prescribed by our team, guided by your labs and your goals, and matched to the right protocol for you. If you are wondering whether this one fits where you want to go, our peptide therapy program in Atlanta is the place to start.
